
- Information
- AI Chat
NSG233 Exam 1 Study Guide Final (1) (1) - Copy
Med-Surg III (NSG 233)
Herzing University
Recommended for you




Preview text
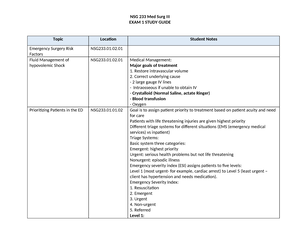
Med Surg III EXAM 1 STUDY GUIDE Topic Location Student Notes Emergency Surgery Risk Factors
NSG 233 .01.
Fluid Management of hypovolemic Shock
NSG 233 .01.
Prioritizing Patients in the ED NSG 233 .01. Violence in the ED NSG 233 .01. Family Focused Interventions NSG 233 .01. Caring for Emergency Personnel
NSG 233 .01.
Complications of rapid IV infusions
NSG 233 .03.01 3
Drugs used in bronchoscopy NSG 233 .01. Priority actions for hemorrhage
NSG 233 .01.
Reversal agents of anticoagulants
NSG 233 .01.
Heat Exhaustion NSG 233 .01. Frostbite NSG 233 .01. Suture Care NSG 233 .01. Hypothermia Interventions NSG 233 .01. Decompression Sickness NSG 233 .01. Nonfatal Drowning NSG 233 .01. Antivenin administration NSG 233 .01.03 4 most effective if given within 4 hours and no greater than 12 hours after the snakebite. The decision to administer antivenin depends on worsening tissue injury and evidence of systemic and coagulopathic symptoms. Rattlesnakes are more likely to cause coagulation abnormalities as well as more systemic effects.
Crotalidae polyvalent immune Fab antivenom (FabAV or CroFab). The dose depends on the type of snake and the estimated severity of the bite. Indications for antivenin depend on the progression of symptoms, including coagulopathy and systemic reaction. does not require pretesting (i., skin sensitivity screening for an allergic reaction, albeit monitoring for a hypersensitivity reaction is still necessary. If the dose exceeds 10 vials, serum sickness will most likely occur. Serum sickness is a type of hypersensitivity response that results in fever, arthralgias, pruritus, lymphadenopathy, and proteinuria and can progress to neuropathies. Caution in pts on anticoag therapy. Before administering antivenin and every 15 minutes thereafter, the circumference of the affected part is measured. Premedication with diphenhydramine or cimetidine may be indicated, because these antihistamines may decrease the allergic response to antivenin. Antivenin is given as an IV infusion whenever possible, although intramuscular administration can be used. Depending on the severity of the snakebite, the antivenin is diluted in 500 to 1000 mL of normal saline solution. The infusion is started slowly, and the rate is increased after 10 minutes if there is no reaction. The total dose should be infused during the first 4 to 6 hours after the bite. The initial dose is repeated until symptoms decrease, after which time the circumference of the affected part should be measured every 30 to 60 minutes for the next 48 hours to detect symptoms of compartment syndrome most common cause of allergic reaction to the antivenin is too-rapid infusion. Reactions may consist of a feeling of fullness in the face, urticaria, pruritus, malaise, and apprehension. These symptoms may be followed by tachycardia, shortness of breath, hypotension, and shock. In this situation, the infusion should be stopped immediately and IV diphenhydramine given. Vasopressors are used for patients in shock, and resuscitation equipment must be on standby while antivenin is infusing. It is important to note that serum
Alcohol withdrawal treatments
NSG 233 .01.
Treatment of suspected Intimate Partner violence
NSG 233 .01 4.
Triage Patients in the ED NSG 233 .01.01 2 Medications for the management of sexual assault
NSG 233 .01.
Care of patients with violent behavior
NSG 233 .01.
Pneumothorax care NSG 233 .02.01 Tension pneumothorax requires needle decompression followed by chest tube insertion Pneumothorax Education NSG 233 .02. Pneumothorax care NSG 233 .02. Medication Math NSG 233 .01. Patient Controlled Analgesia NSG 233 .02. Crush Injuries NSG 233 .02.02 • Risk for: - Rhabdomyolysis (Crush Syndrome) - Destroyed skeletal muscle cells empty contents into circulation - Muscle pain, muscle weakness, elevated CK, dark brown urine - Can lead to acute renal failure - Primary treatment: fluid therapy - Compartment Syndrome - Increased pressure within muscle compartments - Extreme pain, decreased or absent CMS - Leads to decreased perfusion → loss of limb - Primary treatment: fasciotomy Crush injuries NSG 233 .02.02 Rhabdomyolysis->Myoglobinuria Thirds space->Hypovolemic Shock Metabolic abnormalities->VFib DIC-> Coag probs & acute kidney failure most of the time it’s the Lower extremities. Treatment of shock NSG 233 .03.
Stages of Shock NSG 233 .03. Assessing Septic shock NSG 233 .03. Prioritizing orders in the care of sepsis
NSG 233 .03.
Prioritizing orders in the care of Hypovolemic Shock
NSG 233 .03.
Assessing Flail Chest NSG 233 .02. Assessing Septic Shock NSG 233 .03. Assessing Hypovolemic Shock NSG 233 .03. Topic Location Student Notes Assessing Neurogenic Shock NSG 233 .03. Care of Septicemia NSG 233 .03. Medications used to treat Neurogenic and Anaphylactic Shock.
NSG 233 .03.
Assessing MODS NSG 233 .03. Medications used to treat Neurogenic and Anaphylactic Shock
NSG 233 .03 2 .0 4
Treating cardiogenic shock NSG 233 .03. Medications used to treat hypovolemic and cardiogenic shock
NSG 233 .03.
Assessing wounds NSG 233 .01.02 1 Statins help w pain and you have to monitor CK and the adverse effect is that they cause rhabodyalsis
NSG233 Exam 1 Study Guide Final (1) (1) - Copy
Course: Med-Surg III (NSG 233)
University: Herzing University






