
- Information
- AI Chat
Fundamentals of Nursing - Ch. 41 Oxygenation - RN Nclex
Adult Health II (NUR 2211)
Hillsborough Community College
Recommended for you



Students also viewed
- Fundamentals of Nursing - Ch. 40 Hygiene - RN Nclex
- Saunders Vital Signs and Laboratory Reference Intervals RN Nclex
- Saunders Parenteral Nutrition RN Nclex
- Saunders Acid-Base Balance RN Nclex
- Saunders Ch. 6 Ethical and Legal Issues RN Nclex
- Saunders 7th Edition Integumentary Disorders of the Adult Client : Integumentary System RN Nclex
Related documents
Preview text
Oxygenation
OBJECTIVES
- Describe the structure and function of the cardiopulmonary system.
- Describe the physiological processes of ventilation, perfusion, and exchange of respiratory gases.
- Differentiate among the physiological processes of cardiac output, myocardial blood flow, and systemic circulation.
- Describe the relationship of cardiac output (preload, afterload, contractility, and heart rate) to the process of oxygenation.
- Identify the potential clinical outcomes occurring as a result of hyperventilation, hypoventilation, and/or hypoxemia.
- Identify the potential clinical outcomes occurring as a result of disturbances in conduction, altered cardiac output, impaired valvular function, myocardial ischemia, and/or impaired tissue perfusion.
- Describe the effect of a patient’s level of health, age, lifestyle, and environment on oxygenation.
- Describe how to assess for the risk factors affecting a patient’s oxygenation.
- Describe how to assess for the physical manifestations that occur with alterations in oxygenation.
- Develop a plan of care for a patient with altered oxygenation.
- Describe nursing care interventions used to promote oxygenation in the primary care, acute care, and restorative and continuing care settings.
- Describe strategies to use to maintain a patient’s airway.
- Evaluate a patient’s responses to oxygenation therapies.
KEY TERMS
- Acute coronary syndrome (ACS), p.
- Afterload, p.
- Angina pectoris, p.
- Bilevel positive airway pressure (BiPAP), p.
- Bronchoscopy, p.
- Capnography, p.
- Cardiac output, p.
- Cardiopulmonary rehabilitation, p.
- Cardiopulmonary resuscitation (CPR), p.
- Chest physiotherapy (CPT), p.
- Chest tube, p.
- Cheyne-Stokes respiration, p.
- Continuous positive airway pressure (CPAP), p.
- Diaphragmatic breathing, p.
- Diffusion, p.
- Electrocardiogram (ECG), p.
- Endotracheal (ET) tube, p.
- Hematemesis, p.
- Hemoptysis, p.
- Hemothorax, p.
- Humidification, p.
- Hyperventilation, p.
- Hypoventilation, p.
- Hypovolemia, p.
- Hypoxia, p.
- Incentive spirometry, p.
- Invasive mechanical ventilation, p.
- Kussmaul respiration, p.
- Myocardial infarction (MI), p.
- Myocardial ischemia, p.
Scientific Knowledge Base
Oxygen is a basic human need. The cardiac and respiratory systems work together to supply the body with oxygen necessary for carrying out the respiratory and metabolic processes needed to sustain life. Blood is oxygenated through the mechanisms of ventilation, perfusion, and transport of respiratory gases. Neural and chemical regulators control the rate and depth of respiration in response to changing tissue oxygen demands. The cardiovascular system provides the transport mechanisms to distribute oxygen to cells and tissues of the body (McCance and Huether, 2019).
Respiratory Physiology
Respiration is the exchange of oxygen and carbon dioxide during cellular metabolism. It is commonly confused as the act of air moving in and out of the lungs, which is actually ventilation. The airways of the lung transfer oxygen from the atmosphere to the alveoli, where the oxygen is exchanged for carbon dioxide (CO 2 ). Through the alveolar capillary membrane,
oxygen transfers to the blood, and CO 2 transfers from the blood to the
alveoli. There are three steps in the process of oxygenation: ventilation, perfusion, and diffusion (McCance and Huether, 2019).
Structure and Function
The respiratory muscles, pleural space, lungs, and alveoli are essential for ventilation, perfusion, and exchange of respiratory gases. Gases move into and out of the lungs through pressure changes. Intrapleural pressure is negative, or less than atmospheric pressure, which is 760 mm Hg at sea level. For air to flow into the lungs, intrapleural pressure becomes more negative, seing up a pressure gradient between the atmosphere and the alveoli. The diaphragm and external intercostal muscles contract (move downward and outward) to create a negative pleural pressure and increase the size of the thorax for inspiration. Relaxation of the diaphragm and contraction of the internal intercostal muscles allow air to escape from the lungs (Cedar, 2018; McCance and Huether, 2019). Ventilation is the process of moving gases into and out of the lungs with air flowing into the lungs during inhalation (inspiration) and out of the lungs during exhalation (expiration). It requires coordination of the muscular and elastic properties of the lungs and thorax. The major
inspiratory muscle of respiration is the diaphragm. It is innervated by the phrenic nerve, which exits the spinal cord at the fourth cervical vertebra. Perfusion relates to the ability of the cardiovascular system to pump oxygenated blood to the tissues and return deoxygenated blood to the lungs. Finally, diffusion is responsible for moving the respiratory gases from one area to another by concentration gradients. For the exchange of respiratory gases to occur, the organs, nerves, and muscles of respiration need to be intact and the central nervous system needs to be able to regulate the respiratory cycle (Cedar, 2018; McCance and Huether, 2019). Conditions or diseases that change the structure and function of the pulmonary system alter respiration. Some of these conditions include chronic obstructive pulmonary disease (COPD), asthma, lung cancer, and cystic fibrosis. In these conditions, you could find increased respiratory rate, decreased oxygen saturation levels, or adventitious lung sounds (McCance and Huether, 2019).
Work of Breathing
Work of breathing (WOB) is the effort required to expand and contract the lungs. In the healthy individual breathing is quiet and accomplished with minimal effort. The amount of energy expended on breathing depends on the rate and depth of breathing, the ease in which the lungs can be expanded (compliance), and airway resistance (McCance and Huether, 2019 ). Inspiration is an active process, stimulated by chemical receptors in the aorta. Expiration is a passive process that depends on the elastic recoil properties of the lungs, requiring lile or no muscle work. Surfactant is a chemical produced in the lungs to maintain the surface tension of the alveoli and keep them from collapsing. Patients with advanced COPD lose the elastic recoil of the lungs and thorax. As a result, the patient’s work of breathing increases. In addition, patients with certain pulmonary diseases have decreased surfactant production and sometimes develop atelectasis. Atelectasis is a collapse of the alveoli that prevents normal exchange of oxygen and carbon dioxide (McCance and Huether, 2019). Accessory muscles of respiration (the intercostal muscles in the rib cage and abdominal muscles) can increase lung volume during inspiration. Patients with COPD, especially emphysema, frequently use these muscles to increase lung volume. Prolonged use of the accessory muscles does not promote effective ventilation and eventually causes fatigue. During assessment a patient’s clavicles may elevate during inspiration, which can
arterioles to the pulmonary capillaries, where blood comes in contact with the alveolar capillary membrane and the exchange of respiratory gases occurs. The oxygen-rich blood then circulates through the pulmonary venules and pulmonary veins, returning to the left atrium (McCance and Huether, 2019).
Respiratory Gas Exchange
Diffusion is the process for the exchange of respiratory gases in the alveoli of the lungs and the capillaries of the body tissues. Diffusion of respiratory gases occurs at the alveolar capillary membrane (Fig. 41). The thickness of the membrane affects the rate of diffusion. Increased thickness of the membrane impedes diffusion because gases take longer to transfer across the membrane. Patients with pulmonary edema, pulmonary infiltrates, or pulmonary effusion have a thickened membrane, resulting in slow diffusion, slow exchange of respiratory gases, and decreased delivery of oxygen to tissues. Chronic diseases (e., emphysema), acute diseases (e., pneumothorax), and surgical processes (e., lobectomy) often alter the amount of alveolar capillary membrane surface area (McCance and Huether, 2019).
FIG. 41 Alveoli at terminal end of lower airway. From Patton KT, Thibodeau GA: Human body in health and disease, ed 7, St Louis, 2018, Elsevier.
Oxygen Transport
The oxygen-transport system consists of the lungs and cardiovascular system. Delivery depends on the amount of oxygen entering the lungs (ventilation), blood flow to the lungs and tissues (perfusion), rate of
Cardiovascular Physiology
Cardiopulmonary physiology involves delivery of deoxygenated blood (blood high in carbon dioxide and low in oxygen) to the right side of the heart and then to the lungs, where it is oxygenated. Oxygenated blood (blood high in oxygen and low in carbon dioxide) then travels from the lungs to the left side of the heart and the tissues. The cardiac system delivers oxygen, nutrients, and other substances to the tissues and facilitates the removal of cellular metabolism waste products by way of blood flow through other body systems such as respiratory, digestive, and renal (McCance and Huether, 2019).
Structure and Function
The right ventricle pumps deoxygenated blood through the pulmonary circulation (Fig. 41). The left ventricle pumps oxygenated blood through the systemic circulation. As blood passes through the circulatory system, there is an exchange of respiratory gases, nutrients, and waste products between the blood and the tissues. Alterations in structure and function of the heart can lead to a variety of symptoms, including but not limited to dyspnea, edema, and weak pulses. Nurses hear abnormal heart sounds, such as murmurs or rubs, when the structure of the heart is altered (McCance and Huether, 2019).
FIG. 41 Schematic representation of blood flow through the heart. Arrows indicate direction of flow and pulmonary circulation. Modified from Lewis SM, et al: Medical surgical nursing: assessment and management of clinical problems, ed 10, St Louis, 2017, Mosby.
Myocardial Pump
The pumping action of the heart is essential to oxygen delivery. There are four cardiac chambers: two atria and two ventricles. The ventricles fill with blood during diastole and empty during systole. The volume of blood ejected from the ventricles during systole is the stroke volume. Hemorrhage and dehydration cause a decrease in circulating blood volume and a decrease in stroke volume (McCance and Huether, 2019). Myocardial fibers have contractile properties that allow them to stretch during cardiac filling. In a healthy heart this stretch is proportionally related to the strength of contraction. As the myocardium stretches, the strength of the subsequent contraction increases; this is known as the Frank-Starling (Starling’s) law of the heart. In the diseased heart
These arteries branch into smaller arteries; then arterioles; and finally, the smallest vessels, the capillaries. The exchange of respiratory gases occurs at the capillary level, where the tissues are oxygenated. The waste products exit the capillary network through venules that join to form veins. These veins become larger and form the vena cava, which carry deoxygenated blood back to the right side of the heart, where it then returns to the pulmonary circulation (McCance and Huether, 2019).
Blood Flow Regulation
The amount of blood ejected from the left ventricle each minute is the cardiac output. The normal cardiac output is 4 to 8 L/min in the healthy adult at rest. The circulating volume of blood changes according to the oxygen and metabolic needs of the body. For example, cardiac output increases during exercise, pregnancy, and fever but decreases during sleep. The following formula represents cardiac output:
Stroke volume is the amount of blood ejected from the ventricle with each contraction. The normal range for a healthy adult is 50 to 75 mL per contraction. Preload, afterload, and myocardial contractility all affect stroke volume. Preload is the amount of blood in the left ventricle at the end of diastole, before the next contraction. It is often referred to as end- diastolic volume. The ventricles stretch when filling with blood. The more stretch on the ventricular muscle, the greater the contraction and the greater the stroke volume (Starling’s law). In certain clinical situations, medical treatment alters preload and subsequent stroke volumes by changing the amount of circulating blood volume. For example, when treating a patient who is hemorrhaging, increased fluid therapy and replacement of blood increase circulating volume, thus increasing the preload and stroke volume, which in turn increases cardiac output. If volume is not replaced, preload, stroke volume, and the subsequent cardiac output decrease (McCance and Huether, 2019). Afterload is the resistance to the ejection of blood from the left ventricle. The heart works harder to overcome the resistance so that blood can be ejected from the left ventricle. The diastolic aortic pressure is a good
clinical measure of afterload. In hypertension, the afterload increases, causing an increase in cardiac workload (McCance and Huether, 2019). Myocardial contractility is the ability of the heart to squeeze blood from the ventricles. It also affects stroke volume and cardiac output. Poor ventricular contraction decreases the amount of blood ejected. Injury to the myocardial muscle, such as an acute MI, causes a decrease in myocardial contractility (McCance and Huether, 2019). The myocardium in some older adults is stiffer with a slower ventricular filling rate and prolonged contraction time (Touhy and Je, 2018). Heart rate affects blood flow because of the relationship between heart rate and diastolic filling time. For example, a sustained heart rate greater than 160 beats/min decreases diastolic filling time, which decreases stroke volume and cardiac output (McCance and Huether, 2019). The heart rate of the older adult is slow to increase under stress, but studies have found that this may be caused more by lack of conditioning than age. Exercise is beneficial in maintaining function at any age (Touhy and Je, 2018).
Conduction System
The rhythmic relaxation and contraction of the atria and ventricles depend on continuous, organized transmission of electrical impulses. The cardiac conduction system generates and transmits these impulses (Fig. 41).
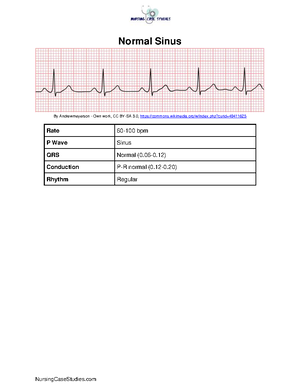
An electrocardiogram (ECG) is a measurement of the electrical activity of the conduction system. An ECG monitors the regularity and path of the electrical impulse through the conduction system; however, it does not reflect the muscular work of the heart. The normal sequence on the ECG is called the normal sinus rhythm (NSR) (see Fig. 41) (Urden et al., 2020). NSR implies that the impulse originates at the SA node and follows the normal sequence through the conduction system. The P wave (atrial depolarization) represents the electrical conduction through both atria. Atrial contraction follows the P wave. The PR interval represents the impulse travel time from the SA node through the AV node, through the bundle of His, and to the Purkinje fibers. The normal length for the PR interval is 0 to 0 seconds. An increase in the time greater than 0. seconds indicates a block in the impulse transmission through the AV node, whereas a decrease, less than 0 seconds, indicates the initiation of the electrical impulse from a source other than the SA node (Urden et al., 2020 ). The QRS complex (ventricular depolarization) indicates that the electrical impulse traveled through the ventricles. Normal QRS duration is 0 to 0 seconds. An increase in QRS duration indicates a delay in conduction time through the ventricles. Ventricular contraction usually follows the QRS complex (Urden et al., 2020). The QT interval represents the time needed for ventricular depolarization and repolarization. The normal QT interval is 0 to 0. seconds. This interval varies inversely with changes in heart rate. Changes in electrolyte values, such as hypocalcemia or hypomagnesemia, or therapy with medications (disopyramide, amiodarone, haloperidol, and azithromycin are examples) increases the QT interval. An increased QT interval increases the person’s risk for lethal dysrhythmias (Urden et al., 2020 ).
Factors Affecting Oxygenation
Four factors influence adequacy of circulation, ventilation, perfusion, and transport of respiratory gases to the tissues: (1) physiological, (2) developmental, (3) lifestyle, and (4) environmental. The physiological factors are discussed here, and the others are discussed in the Nursing Knowledge Base section that follows.
Physiological Factors
Any condition affecting cardiopulmonary functioning directly affects the ability of the body to meet oxygen demands. Respiratory disorders include hyperventilation, hypoventilation, and hypoxia. Cardiac disorders include disturbances in conduction, impaired valvular function, myocardial hypoxia, cardiomyopathy conditions, and peripheral tissue hypoxia. Other physiological processes affecting a patient’s oxygenation include alterations affecting the oxygen-carrying capacity of blood (anemia), decreased inspired oxygen concentration, increases in the metabolic demand of the body (fever), and alterations affecting chest wall movement caused by musculoskeletal abnormalities or neuromuscular alterations (muscular dystrophy) (McCance and Huether, 2019; Urden et al., 2020).
Decreased Oxygen-Carrying Capacity
Hemoglobin carries the majority of oxygen to tissues. Anemia and inhalation of toxic substances decrease the oxygen-carrying capacity of blood by reducing the amount of available hemoglobin to transport oxygen. Anemia (e., a lower-than-normal hemoglobin level) is a result of decreased hemoglobin production, increased red blood cell destruction, and/or blood loss. Patients have fatigue, decreased activity tolerance, increased breathlessness, increased heart rate, and pallor (especially seen in the conjunctiva of the eye). Oxygenation decreases as a secondary effect with anemia. The physiological response to chronic hypoxemia is the development of increased red blood cells (polycythemia). This is the adaptive response of the body to increase the amount of hemoglobin and the available oxygen-binding sites (Lewis et al., 2017; McCance and Huether, 2019). Carbon monoxide (CO) is a colorless, odorless gas that causes decreased oxygen-carrying capacity of blood. In CO toxicity, hemoglobin strongly binds with CO, creating a functional anemia. Because of the strength of the bond, CO does not easily dissociate from hemoglobin, making hemoglobin unavailable for oxygen transport. People with CO poisoning are often unaware of their exposure to this gas, and the symptoms of CO poisoning (headache, dizziness, nausea, vomiting, and dyspnea) mimic other illnesses (Urden et al., 2020).
Hypovolemia
Conditions such as shock and severe dehydration cause extracellular fluid loss and reduced circulating blood volume, or hypovolemia. Decreased circulating blood volume results in hypoxia to body tissues. With
pregnancy, the inspiratory capacity declines, resulting in dyspnea on exertion and increased fatigue (Ball et al., 2019).
Obesity
Patients who are morbidly obese have reduced lung volumes from the heavy lower thorax and abdomen, particularly when in the recumbent and supine positions. Many morbidly obese patients suffer from obstructive sleep apnea. Morbidly obese patients have a reduction in lung and chest wall compliance as a result of encroachment of the abdomen into the chest, increased WOB, and decreased lung volumes. In some patients an obesity- hypoventilation syndrome develops in which oxygenation is decreased and carbon dioxide is retained. The obese patient is also susceptible to atelectasis or pneumonia after surgery because the lungs do not expand fully and the lower lobes retain pulmonary secretions (McCance and Huether, 2019).
Musculoskeletal Abnormalities
Musculoskeletal impairments in the thoracic region reduce oxygenation. Such impairments result from abnormal structural configurations, trauma, muscular diseases, and diseases of the central nervous system. Abnormal structural configurations impairing oxygenation include those affecting the rib cage, such as pectus excavatum, and the vertebral column, such as kyphosis, lordosis, or scoliosis (Ball et al., 2019; McCance and Huether, 2019 ).
Trauma
Flail chest is a condition in which multiple rib fractures cause chest wall instability. This instability allows the lung under the injured area to contract on inspiration and bulge on expiration, resulting in hypoxia. Patients with thoracic or upper abdominal surgical incisions use shallow respirations to avoid pain, which also decreases chest wall movement. Opioids used to treat pain depress the respiratory center, further decreasing respiratory rate and chest wall expansion (Urden et al., 2020).
Neuromuscular Diseases
Neuromuscular diseases affect tissue oxygenation by decreasing a patient’s ability to expand and contract the chest wall. Ventilation is impaired, resulting in atelectasis, hypercapnia, and hypoxemia. Examples of conditions causing hypoventilation include myasthenia gravis and Guillain-Barré syndrome (McCance and Huether, 2019).
y Central Nervous System Alterations
Diseases or trauma of the medulla oblongata and/or spinal cord result in impaired ventilation. When the medulla oblongata is affected, neural regulation of ventilation is impaired, and abnormal breathing paerns develop. Cervical trauma at C3 to C5 usually results in paralysis of the phrenic nerve. When the phrenic nerve is damaged, the diaphragm does not descend properly, thus reducing inspiratory lung volumes and causing hypoxemia. Spinal cord trauma below the C5 vertebra usually leaves the phrenic nerve intact but damages nerves that innervate the intercostal muscles, preventing anteroposterior chest expansion.
Influences of Chronic Lung Disease
Oxygenation decreases as a direct consequence of chronic lung disease. Changes in the anteroposterior diameter of the chest wall (barrel chest) occur because of overuse of accessory muscles and air trapping in COPD or cystic fibrosis. Chronic lung disease often results in varying degrees of dyspnea, tachypnea, hypoxemia and/or hypercapnia (Ball et al., 2019; Lewis et al., 2017; McCance and Huether, 2019).
Alterations in Respiratory Functioning
Illnesses and conditions affecting ventilation or oxygen transport alter respiratory functioning. The three primary alterations are hypoventilation, hyperventilation, and hypoxia. The goal of ventilation is to produce a normal arterial carbon dioxide tension (PaCO 2 ) between 35 and 45 mm Hg and a normal arterial oxygen
tension (PaO 2 ) between 80 and 100 mm Hg. Hypoventilation and
hyperventilation are often determined by arterial blood gas analysis (McCance and Huether, 2019). Hypoxemia refers to a decrease in the amount of arterial oxygen. Nurses monitor arterial oxygen saturation (SpO 2 ) using a pulse oximeter, a noninvasive oxygen saturation monitor.
Normally SpO 2 is greater than or equal to 95% (see Chapter 30).
Hypoventilation
Hypoventilation occurs when alveolar ventilation is inadequate to meet the oxygen demand of the body or eliminate sufficient carbon dioxide. As alveolar ventilation decreases, the body retains carbon dioxide. For example, atelectasis, a collapse of the alveoli, prevents normal exchange of
Fundamentals of Nursing - Ch. 41 Oxygenation - RN Nclex
Course: Adult Health II (NUR 2211)
University: Hillsborough Community College


- Discover more from:





Recommended for you
Students also viewed
- Fundamentals of Nursing - Ch. 40 Hygiene - RN Nclex
- Saunders Vital Signs and Laboratory Reference Intervals RN Nclex
- Saunders Parenteral Nutrition RN Nclex
- Saunders Acid-Base Balance RN Nclex
- Saunders Ch. 6 Ethical and Legal Issues RN Nclex
- Saunders 7th Edition Integumentary Disorders of the Adult Client : Integumentary System RN Nclex