- Information
- AI Chat
Cc 0 orientation - EKG and Hemodynamics
Critical Care (408)
Loma Linda University



Preview text
Normal Breath Sounds inspiration > expiration low pitch soft no adventitious sounds
Vesicular Breath Sound most of lung field low pitch soft & short exhalation long inhalation
Bronchovesicular Breath heard over main bronchus upper right posterior lung field medium pitch exhalation = inhalation
Bronchial Breath Sound trachea only high pitch loud and long exhalation
Crackles excessive secretions/fluid in airway short, discrete popping/crackling sounds associated w/ PNA, pulmonary edema, pulmonary fibrosis, atelectasis
Wheezes vibrations when air flows at fast speed through narrow airway high-pitched, squeaking, whistling sound associated w/ asthma or bronchospasm
Pleural Friction Rub produced by irritated pleural surfaces rubbing together creaking, leathery, dry, coarse, sound associated w/ pleural effusion, pleurisy
Absent no airflow to particular portion of lung associated w/ pneumothorax, pneumonectomy, lung mass, complete airway obstruction
Diminished little airflow to particular portion of lung sound intensity is reduced associated w/ atelectasis, COPD, obesity
Stridor sign of obstruction in trachea or larynx loud, high-pitched sound (sounds like snore) wake pt. up to r/o stridor if awake & still has snoring sound positive for stridor Chest Tube Nursing Actions Chest Tube always keep drainage system below level of chest & free of kinks troubleshoot cause if there’s change in previous assessment if cause can’t be confirmed notify physician ALWAYS have sterile Vaseline gauze on hand in case of accidental dislodgement if chest tube comes off apply pressure on insertion site w/ sterile Vaseline gauze and call physician
Value of ScvO remove fluid & air from pleural space three chest tube settings suction water seal (to gravity) clamped assessed if pt. can tolerate function without chest tube or if they don’t need chest tube anymore air leaks bubbling in the drainage system assess and identify cause every shift
central venous oxygen saturation normal: 70 – 80% ScvO2 can be used as convenient surrogate to a PA catheter for detection & rapid TX of tissue hypoxia sustained ScvO2 <70% associated w/ higher mortality
Arterial Line (A-line, ABP) Central Venous Catheter (triple lumen CVC, CVL)
Pulmonary Artery Catheter
continuous monitoring of ABP non-traumatic sampling of arterial blood gas (ABG) do NOT infuse
continuous monitoring of central venous pressure monitoring of central venous oxygen saturation (ScvO2)
reserved for most hemodynamically unstable patients for diagnosis & evaluation of heart dz, pulmonary HTN, shock
medications/IV in A-line Mean Arterial Pressure (MAP) normal: 70-100mmHg mean > 60 to perfuse vital organs MAP = [ 2(diastolic) + systolic] ÷ 3 arterial waveform in EKG dicrotic notch (aortic valve closing little back pressure bump) & appropriate waveform for each QRS highest point = SBP, lowest point = DBP
fluid/volume status monitoring, blood draws, meds, IV fluid Central Venous Pressure measures right atrial pressure (PRELOAD) reflects force-filling of R atrium & R ventricle measured at junction of vena cava and Rt atrium & CVP only measured w/ central line unable to transduce CVP from peripheral or short PICC line normal: 2-5 - indicate fluid balance
states
normal values PAP: 20-30mmHg/5- 10mmHg measured w/ balloon deflated PAOP: 5-12mmHg wedge pressure w/ balloon inflated left ventricle at end diastolic pressure (LVEDP) CO: 4-6L/min
Zeroing a Line level transducer @ phlebostatic axis (4th ICS, MAL) close stopcock to patient open transducer to air press “zero” on monitor/touchscreen close transducer to air open stopcock to patient quick flush of line (square test)
Nursing Care on A- Line, CVC, PA maintain pressure bag at 300mmHg maintain gravity infusion at 3mL/hr change heparin/saline flush solution bag q24h or when it runs out change pressure tubing q48-72h (2-3days) per unit protocol assess site & change dressing per protocol assess if pressure readings & waveforms are normal or abnormal run EKG strips of waveform & place on chart every shift
Central Line Complications phlebitis at insertion site air embolism hematoma arrhythmia catheter malposition late complications thrombus formation infection
External Ventricular Device (EVD) measures ICP & drain CSF indicated in intracranial hemorrhage, traumatic brain injury, bacterial meningitis most common/important lifesaving procedures in neuro ICU subarachnoid screw EVD normal: 4-15mmHg slightly elevated: 15- 20mmHg if >20mmHg for 10mins NOTIFY PROVIDER
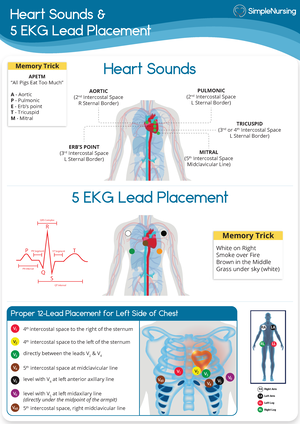
Heart Sounds S1 (lubb) mitral & tricuspid valves (AV) close high pitched “lubb” sound loudest at apex beginning of systole isometric contraction
S
aortic & pulmonic valves (semilunar) close high pitched “dubb” sound loudest at base end of systole & beginning of diastole isometric
S
rapid filling of ventricles in early diastole low pitched Kentucky | “what the heck” normal in children and pts w/ high ↑ CO pregnant mom, athletes) pathological in
S
sign of diastolic heart failure (late diastole) Tennessee | bad joke drum active ischemia chronic HTN ( syllables – S4) left ventricular hypertrophy (LVH) impaired relaxation
aortic = 2nd ICS on Rt chest pulmonic = 2nd ICS on Lt chest erb’s point = 3rd ICS tricuspid = 4th/5th ICS mitral = 5th ICS all people enjoy touching me
decrease to 0/min for 18hrs
Cc 0 orientation - EKG and Hemodynamics
Course: Critical Care (408)
University: Loma Linda University