- Information
- AI Chat
Cc 1 normal electrophysiology
Critical Care (408)
Loma Linda University



Related Studylists
211Preview text
Afterload ventricular wall tension during systolic ejection force to get blood out systemic vascular resistance (SVR)
↑ afterload ↑heart
workload SVR ↑ by factors that oppose ejection & anything that affects heart to pump
Contractility = Inotropy heart’s contractile force (how hard heart beats) Cardiac Index (CI) CO based on body size CI = CO/BSA (body surface area) L/min/m 2
Cardiac Output (CO) volume of blood ejected from heart in 1min CO = HR x SV heart rate (HR) = beats per minute stroke volume (SV) = mL of blood ejected from heart in one beat normal CO = 4-8L/min (4-6L/min at rest)
Sinoatrial (SA) Node intrinsic/normal pacemaker 60-100 beats per minute
Atrioventricular (AV) Node secondary pacemaker if SA node fails AV node kicks in as first backup slight pause 40-60 beats per minute
Purkinje Fiber last chance if SA and AV node fails purkinje fibers kick in as second backup 15-40 beats per minute
Automaticity ability of certain cells to spontaneously depolarize (pacemaker potential) Excitability given stimulus depolarize in response Conductivity transmit a stimulus from cell to cell Rhythmicity automatic generated at a regular rate Contractility depolarization cardiac myofibrils shorten in length Refractoriness state of cell/tissue during repolarization tissue can’t depolarize regardless of intensity of stimulus or requires a much greater stimulus than normally required
potassium (K+) intra > extra (more inside cell) sodium (Na+) intra < extra (more outside cell) calcium (Ca2+) intra < extra (more outside cell)
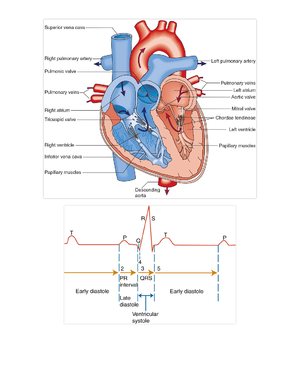
Phases of Action Potential Phase 0 - Depolarization fast Na channels open lots of Na goes in action potential charge +20 to +30mV Phase 1 action potential returns to 0mV fast Na channels close Phase 2 - Plateau slow Na & Ca channels open K flows out plateau Ca causes cardiac muscle cell contraction Phase 3 - Repolarization slow Na & Ca channels close K continues to move out reestablish resting membrane potential (RMP) Phase 4 action potential returns to -80 to -90mV Na/K pump work to correct intra/extracellular ion concentrations back to equilibrium
Action Potential depolarization & repolarization moves along cell in wave-like fashion Chemical Gradient move from high to low concentration Electrical Gradient move to area w/ opposite charge Membrane Permeability selectivity of membrane to ionic movement
Intercalated disks anchor points provides rapid transmission of information promote prolongation of action potential Absolute refractory period cell CANNOT be depolarized AT ALL Relative refractory period cell CANNOT FULLY repolarize but could be depolarized if stimulus strong enough peak of T wave = vulnerable to stimuli
Parasympathetic Nervous System (PNS) rest & digest vagus nerve everything ↓ BUT constricts bronchioles & ↑ peristalsis & digestive secretions concentrated near SA/AV nodes slow heart rate Sympathetic Nervous System (CNS) fight or flight follow path of major coronary arteries everything ↑, ↑ HR & contractility
Electrocardiogram (ECG/EKG)
Normal Interval Ranges PR beginning of P wave to beginning of QRS time for electricity to spread from SA to AV node ventricular filling time 0 - 0. QRS ventricular (SA & AV) depolarization 0 – 0 (< 3 small boxes) if widened QRS (>3 small boxes) conduction delay in 1 or both ventricles QT interval ventricular systole accurate end of T wave important slanted line intersects baseline QT 0 – 0. >0 can be d/t hypoK or meds (Seroquel) T wave rapid ventricular repolarization peaked electrical instability d/t e- abnormality (hyperkalemia) inverted (peaks downward below baseline) r/t old infarction or evolving ischemia U wave (SHOULD NOT EXIST) diastolic deflection sometimes seen at end of T wave T-U junction should be at isoelectric line upright U – normal variant prominent w/ hypo noticeable HR <65, never seen when HR >
provides record of cardiac electrical activity & information of heart function & structure Why important? vitals at a glance critical pts change quickly improvement/worsening of pts condition (especially MI & STEMI) monitor for arrhythmias additional tests can be ordered based on EKG EKG paper EKG machine moves at 25mm/sec small box = 0 small box = 1mm large box = 0 5 large boxes = 1 Determine Heart Rate in EKG 6inch strip 6in = 6sec most common esp. irregular rhythm #QRS complexes in strip x 10 between 2 hash marks or 30 big boxes divide 300 by #large boxes between QRS only on regular rhythm divide 1500 by #small boxes between QRS only on regular rhythm Rhythm take calipers peak to peak if they match up = regular one is off (soon or late) = irregular Artifacts ‘shaky’ look on EKG adjust leads & instruct pt to stop movement
EKG - Three Laws of Deflection leads are polarized electricity moving toward positive (+) electrode upright deflection electricity moving away from positive (+) electrode downward deflection electricity moving past positive (+) electrode biphasic complex (upward & downward)
Heartbeat Regulation Baroreceptors aortic arch & carotid sinus sensitive to stretch/pressure sense change in stretch measures stretch stimulate ANS to response to changes Chemoreceptors carotid arteries & bifurcation of aortic arch sensitive to change in chemicals sense changes in O2 and CO2 pressure Natriuretic Peptides myocardial stretch natriuretic peptides secrete for heart failure pts, BNP will secrete in excess because heart tries to contract to compensate atrial myocardium atrial natriuretic peptide (ANP) ventricular myocardium brain natriuretic peptide (BNP) Renin-Angiotensin- Aldosterone System (RAAS) activates by ↓ BP (↓ BF to juxtaglomerular apparatus in kidney) renin angiotensin I angiotensin II vasoconstriction & aldosterone released Na retained water retained ↑BP
peaked p waves P pulmonale happens from COPD cor pulmonale
Block left bundle has 3 parts all 3 parts blocked = LBBB otherwise it’s a hemiblock V1 – final deflection is deep negative V6 – final deflection is tall upright carrots
Block wide QRS V1 – rsR’ V6 – last deflection is negative bunny ears
Cc 1 normal electrophysiology
Course: Critical Care (408)
University: Loma Linda University