
- Information
- AI Chat
ALS cane and crutches
bs nursing
Southwestern University PHINMA
Recommended for you




Preview text
PREPARED BY: SANDRA M. COVARRUBIAS
At the end of the lecture the student will be able to: 1. Purpose of assistive devices. 2. State the indications for ambulating with assistive devices. 3. Define what is cane. 4. State the purpose of using a cane. 5. Describe the three types of canes. 6. Name the basic parts of a cane. 7. Describe three characteristics of appropriately fittedcane. 8. Identify appropriate assessment skills prior to the procedure. 9. Formulate relevant nursing diagnosis related to the procedure/ treatment/ therapy. 10. Demonstrate the step-by-step procedure: Assisting a Patient with Ambulation Using a Cane, stating the rationale for each steps. 11. Describe “moving in and out” of a chair using a cane. 12. Discuss the “going up and down” the stair using a cane.
Due to assistive technology, people with disabilities havean opportunity of a more positive and easygoing lifestyle, with an increase in "social participation," "security and control."
Indication for Assistive Devices Structural deformity, amputation, injury, or disease resulting in decreased ability to weightbear through lower extremities Muscle weakness or paralysis of the trunk or lower extremities Inadequate balance
anes are assistive devices, useful for patients who can bearweight but need support for balance and stability. They are also useful for patients whohave decreased strength in one leg. Canes provide an additional point of support duringambulation and promotes greater independence.
Types of Cane
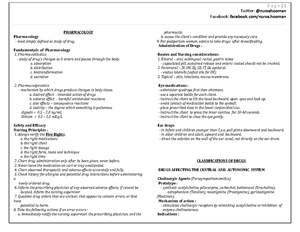
Canes are made of wood or metal and often have a rubberized capon the tip to prevent slipping. Canes come in three variations: standardstraight or single-ended canes with half-circle handles (A), recommended for patients requiring minimal support and for those who will be using stairs frequently; standard straight or single-ended canes with L- shape handles (B), recommended for patients with hand weakness because the handgrip is easier to hold, but not recommended for patients with poor balance; canes with three (tripod) (E) or four legs/tips (quad cane) (F) provide a wide base of support, recommended for patients with poor balance.
C
Figure 1. Types of canes.
The basic cane has four parts
Handle. The handle of a cane is extremely important to the user. Manydifferent styles exist, the most common traditional designs are the Tourist, or crook handle, the Fritz Handle and the Derby Handle. Ergonomically shapedhandles have become increasingly common for canes intended for medical use, both increasing the comfort of the grip for the user (particularly importantfor users with disabilities which also affect their hands or wrists), and better transmitting the load from the user's hand and arm into the shaft. Collar. The collar of a cane may be only a decorative addition made for stylistic reasons, or may form the structural interface between shaftand handle. Shaft. The shaft of the cane transmits the load from the handle to the ferrule and may be constructed fromcarbon fiber polymer, metal, composites, or traditional wood. Ferrule. The tip of a cane provides traction and added support when the cane is used at an angle. Many kinds of ferrules exist, but most common is a simple, ridged rubber stopper. Users can easily replace a ferrule with one that better suits their individual needs.
A. Standard straight wooden cane with half-circle handle. B. Standard straight wooden cane with L-shape handle.
C. Standard straight metal cane with half-circle handle. D. Standard straight metal cane with L-shape handle.
E. Tripod cane F. Quad cane
Figure 3. Fitting the Cane.
Try This!
Equipment:
Cane of appropriate size with rubber tip Nonskid shoes or slippers Nonsterile gloves and/or other PPE, as indicated Stand-assist aid, if necessary and available Gait belt, based on assessment (figure 4)
ASSESSMENT:
Assess the patient’s upper body strength, ability to bear weight and to walk, and the need for assistance. Review the patient’s record for conditions that may affect ambulation. Perform a pain assessment before the time for the activity. If the patient reports pain, administer the prescribed medication in sufficient time to allow for the full effect of the analgesic. Take vital signs and assess the patient for dizziness or lightheadedness with position changes. Assess the patient’s knowledge regarding the use of a cane.
SKILL 1: ASSISTING A PATIENT WITH AMBULATION USING A
A. Elbow should bend at a comfortable angle, 15-30 degree.
B. Proper height of the cane handle should align with the wrist while standing erect.
Figure 4. Gait Belt is a device used by nurse to transfer patient with mobility issues from one position to another, from one location to another or while assertively ambulating patients who have problems with balance.
NURSING DIAGNOSIS:
Determine the related factors for the nursing diagnosis based on the patient’scurrent status. Appropriate nursing diagnoses may include:
Risk for Falls Activity Intolerance Impaired Walking Acute Pain Deficient Knowledge Chronic Pain Risk for Injury
OUTCOME AND PLANNING:
The expected outcome to achieve when assisting a patient with ambulation usinga cane is that the patient ambulates safely without falls or injury. Additional appropriate outcomes include the following:
the patient demonstrates proper use of the cane; the patient demonstrates increased muscle strength, joint mobility, and independence; the patient exhibits no evidence of injury from use of the cane.
- While supporting his or her weight on the weaker leg and the cane, have the patient advance the stronger leg forward ahead of the cane (heel slightly beyond the tip of the cane).
Moving in this manner provides support and balance.
- Tell the patient to move the weaker leg forward until it is even with the stronger leg, and then advance the cane again.
This motion provides support and balance.
- Continue with ambulation for the planned distance and time.
Continued ambulation promotes activity. Adhering to the planned distance and patient’s tolerance prevents the patient from becoming fatigued.
- Return the patient to the bed or chair based on the patient’s tolerance and condition. Make sure call bell and other necessary items are within easy reach.
Balance activity and rest prevents fatigue and ensures the patient’s comfort.
- Clean transfer aids per facility policy, if not indicated for single patient use. Remove PPE, if used. Perform hand hygiene.
Proper cleaning of equipment between patient use prevents the spread of microorganisms. Removing PPE properly reduces the risk for infection transmission and contamination of other items. Hand hygiene prevents the spread of microorganisms.
EVALUATION:
- Evaluate A. if the patient uses the cane to ambulate safely and is free from falls or injury. B. the patient demonstrates proper use of the cane; C. the patient exhibits increased muscle strength, joint mobility, and independence; and D. the patient experiences no injury related to cane use.
Determines if the expected outcome is met or not, thus needs to be changed.
- Document: A. the activity, any other pertinent observations, B. the patient’s ability to use the cane, C. the patient’s tolerance of the procedure, and the distance walked. D. the use of transfer aids and the number of staff required for transfer.
Provides information with regards to patient’s progress to care and response to therapy.
At the end of the lecture-demonstration the student will be able to:
- Defines what is crutch.
- States the purpose of using crutches.
- Describes the types of crutches, the advantages and disadvantages.
- Names the basic parts of the crutch.
- Describes weight bearing and its types.
- Demonstrates the tripod stance/position when standing with crutches.
- Describes three characteristics of appropriately fitted crutches.
- Identifies and perform the different gait patterns.
- Identifies appropriate assessment skills prior to the procedure.
- Formulates relevant nursing diagnosis related to the procedure/ treatment/therapy.
- Demonstrates the step-by-step procedure: Assisting a Patient with Ambulation Using a Crutches, stating the rationale for each steps.
- Performs moving in and out of the chair with crutches.
- Performs climbing up and going down the stairs
rutch is a mobility aid that transfers weight from the legs to the upper body. It is often used by people who cannot use their legs to support their weight, for reasons ranging from short-term injuries to lifelong disabilities.
Types of Crutches
1. Underarm or axilla crutches
Underarmcrutches are used by placing the pad against the ribcage beneath the armpit and holding the grip, which is below and parallel to the pad. They are usually usedfor short term injuries to provide support for patients who have temporary restriction on ambulation-as in recovering from ankle or knee injuries. Advantages: Underarm crutches are adjustable to a person’s height and come with arm pads and handgrips for comfort. the easiest to use.
Disadvantages This type of crutch people tends to slouch while using them. May causearmpit injury condition known as crutch paralysis, or crutch palsy can arise from pressure on nerves in the armpit, or axilla. Specifically, "the brachial plexus in the axilla is often damaged from the pressure of a crutch.. these cases the radial is the nerve most frequently implicated; the ulnar nerve suffers next in frequency.
c
ASSISTING A PATIENT WITH AMBULATION USING CRUTCHES
Figure 1. Axillary Crutch
Parts of the Crutch
A. B. Figure 5. A. Axillary crutch. B. Forearm crutch
Think Ahead!
GAIT TRAINING: Principles
Weight Bearing is the amount of weight that may be borne on a lower extremity during standing or ambulation isdetermined by patient’s condition and medical management of that condition. Changes in weight bearing status are determined by the patient’s physician.
Types of Weight Bearing
- None Weight Bearing: involved lower extremity not to bear weight or touching floor.
- Toe Touch Weight Bearing: patient can rest toes on the floor for balance, but not to bear weight.
- Partial Weight Bearing: limited amount of weight bearing permitted on lower extremity (example: 25% PWB = 25% of patient’s total body weight is allowed to be transmitted through the involved lower extremity.)
- Weight-Bearing as Tolerated: patient allowed to place as much or as little weight through the involved lower extremity, depending on patient’s tolerance.
- Full Weight-Bearing: The leg can now carry 100% of the body weight, which permits normalwalking.
Standing with Crutches
Tripod Stance is what provides your body with the most support and keeps weight off of your injured leg when standing still. Keep good foot firmly on the ground and place thecrutches in front, crutch tip 6” from the foot and at a 45-degreeangle.
.
ATTENTION! Be careful not to move the crutches too far away or too close tothe body since this will not provide the support you need.
Figure 6. Tripod position.
Measuring for the Crutches
Standard axillary crutches need two adjustments--the length of the crutchand the position of the handgrip. Prior to adjusting, prepare the crutches with padding on the axillary barand a rubber tip on the end of each crutch.
Lying:
Have the patient lie supine, arms at sides, wearing a shoe on the unaffected foot. Using a tape measure, measure from the axilla to the heel of the shoe and add two(2) inches. Adjust the crutch shaft to this measurement. Standing:
Crutch tip 6” from the foot and @ a 450 angle Hand grip @ the ulnar styloid process Elbow in about 20-30 degrees of flexion OR Hand grip @ the level of the greater trochanter Axillary distance to the top of the crutch, 2-3 finger widths
Gait Patterns
1. two-point gait : the client is partially weight-bearing on both legs. (A crutch and the opposite leg are considered one “point.” The other crutch and leg are the second “point.”) Gait speed is faster than 4 point, butless stable as only two points are in contact with floor and good balance is needed to walk with 2 points crutch gait. Low energy required by patient. Pattern: advance right crutch & left foot together, then advance the left crutch & right foottogether. 2. three-point gait, each crutch and only one leg support weight. (Each is considered a “point.”) The other leg is non-weight-bearing. Used when patient has one leg can fully bear weightand one leg can’t bear weight. Most rapid gait speed, provides the least amount of stabilityfor the patient. High energy required by patient.
Figure 7. Gait Patterns.
Try This!
Equipment:
Crutches with axillary pads, hand grips, and rubber suction tips Nonskid shoes or slippers Nonsterile gloves and/or other PPE, as indicated Gait belt
ASSESSMENT
Review the patient’s record and nursing plan of care to determine the reason forusing crutches and instructions for weight bearing. Check for specific instructions from physical therapy. Perform a pain assessment before the time for the activity. If the patient reports pain, administer the prescribed medication in sufficient time to allow for the full effect of theanalgesic. Determine the patient’s knowledge regarding the use of crutches and assess the patient’s ability to balance on the crutches. Assess for muscle strength in the legs and arms. Determine the appropriate gait for the patient to use.
NURSING DIAGNOSIS
Determine the related factors for the nursing diagnosis based on the patient’s current status. Appropriate nursing diagnoses may include:
Risk for Injury Activity Intolerance Impaired Walking Acute Pain or Chronic Pain Deficient Knowledge Risk for Falls
SKILL3: ASSISTING A PATIENT WITH AMBULATION USING
report any feelings of dizziness, weakness, or shortness of breath while walking. Decide how far to walk.
and explanation help allay anxiety and prepare the patient for what to expect.
- Assist the patient to put on appropriate socks and shoes.
- Encourage the patient to make use of the stand-assist device, if available. Assist the patient to stand erect, face forward in the tripod position. This means a. the patient holds the crutches 6- inches in front of and b. 6-12 inches to the side of each footat a 45-degreeangle.
Stand-assist device reduces caregiver strain and decreases risk of patient injury. Positioning the crutches in this manner provides a wide base of support to increase stability and balance.
8. For the four-point gait: a. Begin in the tripod position. b. Have the patient move the right crutch forward 6-12 inches and then move the left foot forward to the level of the right crutch. b. Then have the patient move the left crutch forward 6=12 inches and then move the right foot forward to the level of the left crutch.
This movement ensures stability and safety.
9. For the three-point gait: a. Begin in the tripod position. b. Have the patient move the affected leg and both crutches forward about 6- 12 inches. b. Have the patient move the stronger leg forward to the level of the crutches.
Patient bears weight on the stronger leg.
10. For the swing-to gait: a. Begin in the tripod position. b. Have the patient move both crutches forward about 6-12 inches, c. Have the patient bend and lift the injured leg and swing them at the level of the crutches, d. supporting his or her body weight on the crutches.
Most rapid gait. Patient bears weight on the unaffected leg. Swing-to gait provides mobility for patients with weakness or paralysis of the hips or legs.
11. For the swing-through-gait a. Begin in the tripod position client stands on the strong leg, bending the knee of injured leg. b. Moves both crutches forward the same distance, c. Rests his or her weight on the palms, and swings forward slightly ahead of the crutches.
Most rapid gait. Patient bears weight on the unaffected leg.
12. For the two-point gait: a. Begin in the tripod position. b. Have the patient move the left crutch and the right foot forward about 6- inches at the same time. b. Have the patient move the right crutch
Patient bears partial weight on both feet.
and left leg forward to the level of the left crutch at the same time. 13. Continue with ambulation for the planned distance and time.
Continued ambulation promotes activity. Adhering to the planned distance and time prevents the patient from becoming fatigued.
- Return the patient to the bed or chair based on the patient’s tolerance and condition, ensuring that the patient is comfortable. Make sure call bell and other necessary items are within easy reach.
Provide comfort and prevent fatigue. A call bell reassures the patient that you will attend to his/her needs
- Remove PPE, if used. Perform hand hygiene
Removing PPE properly reduces the risk for infection transmission and contamination of other items. Hand hygiene prevents the spread of microorganisms. EVALUATION 16. Evaluate: a. the patient demonstrates correct use of crutches to ambulate safely and without injury. b. the patient demonstrates increased muscle strength and joint mobility c. Exhibits no evidence of injury related to crutch use.
Determines if the expected outcome is met or not, thus needs to be changed. Determines patient’s progress.
- Document: a. the activity, any other pertinent observations, b. the patient’s ability to use the crutches, the patient’s tolerance of the procedure, and the distance walked. c. Document the use of transfer aids and number of staff required for transfer. d. and other appropriate interventions
Provides information with regards to patient’s progress to care and response to therapy.
Steps in Sitting down and Getting up of the chair
Stand to Sit/ Sitting down:
- Stand in front of the chair with the seat of the chair touching the back of your legs.
- Place both crutches in the hand on the side of your injured leg.
- Place the other hand on the arm rest or side of the chair.
- Sit down and slide back.
Figure 8. Sitting down
Sit to Stand/ Getting up:
- Hold both crutches in the hand on the side of your good leg.
- Slide to the front edge of seat. Both feet flat on the floor (injured leg NWB).
- Place your other hand on the armrest or side of the chair or side of the chair.
- Push yourself up, placing weight on the good leg and the crutches.
- Transfer one crutch to the side of affected leg. Stand in tripod position, before walking.
Figure 8. Getting Up
ALS cane and crutches
Course: bs nursing
University: Southwestern University PHINMA


- Discover more from:bs nursingSouthwestern University PHINMA999+ Documents
- More from:bs nursingSouthwestern University PHINMA999+ Documents


